
Cash and Voucher Assistance works because it’s fundamentally person-centered—it gives people agency and preserves dignity. In the previous article, we projected CVA funding to rebound to $500 million in 2026, cash-based approaches will be central to nearly every national and international NGO’s programming.
As health program professionals who’ve spent three years designing and implementing CVA for health outcomes, here’s our take: if you’re building or scaling CVA programs in 2026, these five elements aren’t optional—they’re essential.
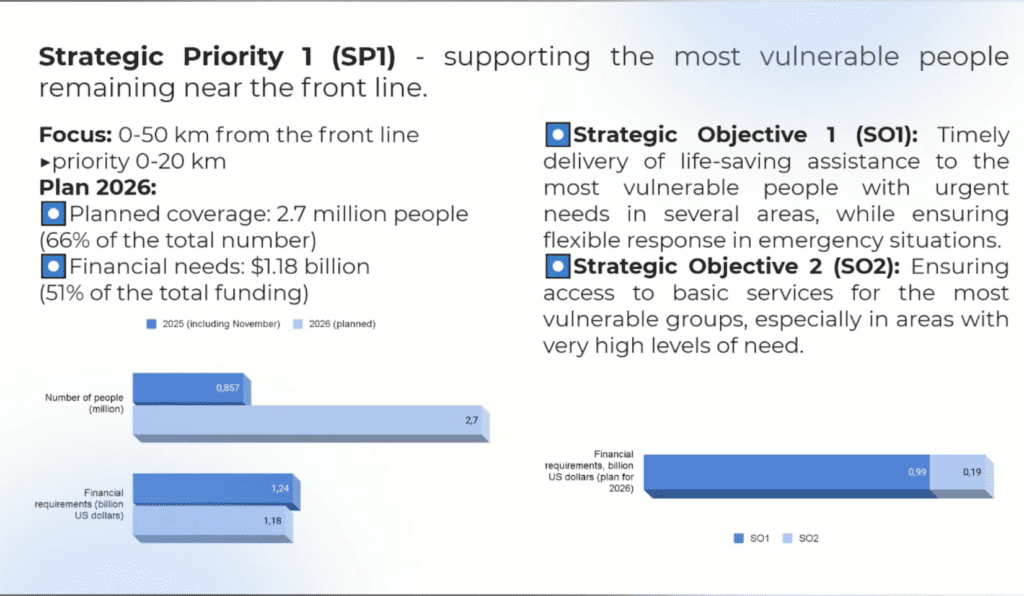
Element 1: Design for the 20km Frontline Zone Reality
Nearly 90% of strikes and more than half of all civilian casualties occur within 20 kilometers of the frontline. Since February 2022, nearly 53,000 civilian casualties have been verified. And it’s getting worse – civilian casualties increased by 27% between January and October 2024 compared to the same period the previous year.
The 2025 is the second after only 2022 by number of civilian casualties in a single year.
Within that 20km belt, entire communities have been devastated. This isn’t about occasional shelling – it’s about systematic destruction of civilian life and infrastructure.
Ask the Right Questions:
When designing programs for the 20km zone, forget the standard playbook. Ask these simple questions:
1. What might be the Cash Transfer modality? Will it be available in the next 6 months?
Banking offices, mobile internet coverage, ATMs, post offices – the infrastructure you take for granted in Kyiv or Lviv might not exist here. Or it might disappear tomorrow.

2. Cash vs. Voucher vs. In-Kind – What Makes Sense?
- Vouchers only work if the service provider is stable for the next 6 months. Can you guarantee that? Think about it.
- In-kind is reliable but creates a huge problem: can people carry it if they need to evacuate suddenly?
- Cash wins in most scenarios because:
- It’s portable during evacuation
- It can buy products vouchers can’t (because services aren’t available)
- People have choice – person-centered approachCash and Voucher Assistance works because it’s fundamentally person-centered—it gives people agency and preserves dignity. After five years of CVA evolution in Ukraine{rel=”nofollow”}, we’ve learned what separates programs that succeed from those that struggle.
- With CVA funding projected to rebound to $500 million in 2026, cash-based approaches will be central to nearly every national and international NGO’s programming. As health program professionals who’ve spent three years designing and implementing CVA for health outcomes, here’s our take: if you’re building or scaling CVA programs in 2026, these five elements aren’t optional—they’re essential.
3. Is the delivery mechanism actually functional?
Check if ATMs work. Look if banks are open. Check if post offices are accessible. These aren’t abstract questions – they determine whether your program works or fails.
Bottom line for the 20km zone: MPCA (Multi-Purpose Cash Assistance) is likely your best bet, but only if you’ve verified the delivery infrastructure exists.
Element 2: Look Beyond Your Comfort Zone
Beginning of the year = time to pivot your geographic focus.
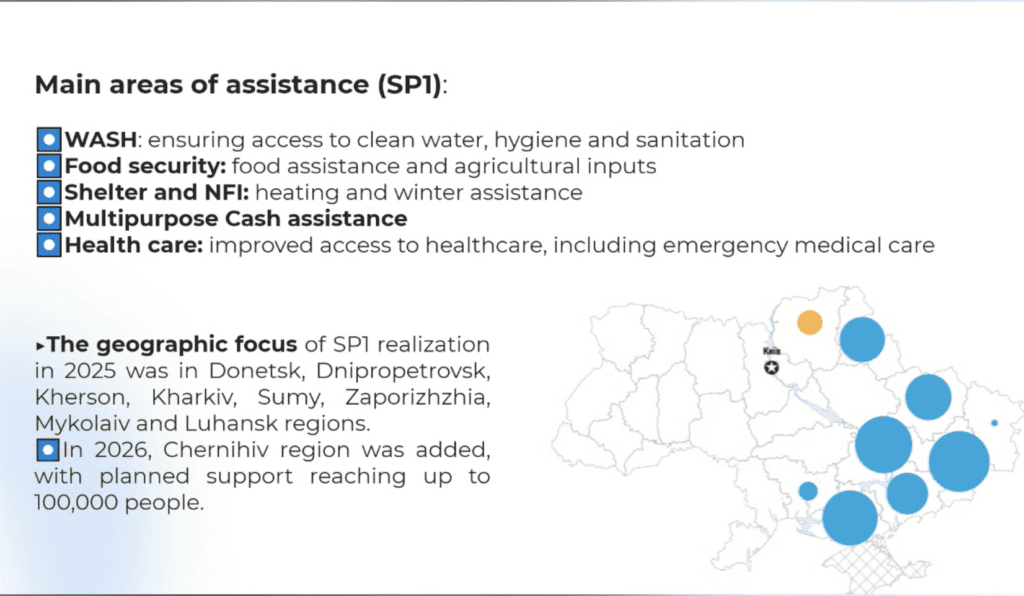
Two oblasts have been criminally underserved since 2022: Sumska and Chernihivska.

These regions border Russia and Belarus. They’re under constant threat of active hostilities. Yet they’ve been off the humanitarian radar for too long. If you’re planning your 2026 program, put Sumy and Chernihiv on your shortlist for MPCA rollout.
Element 3: Prepare for Evacuations and Actually Coordinate
The frontline is unstable. 90% of strikes hit the 20km zone. It will eventually lead to more evacuations.
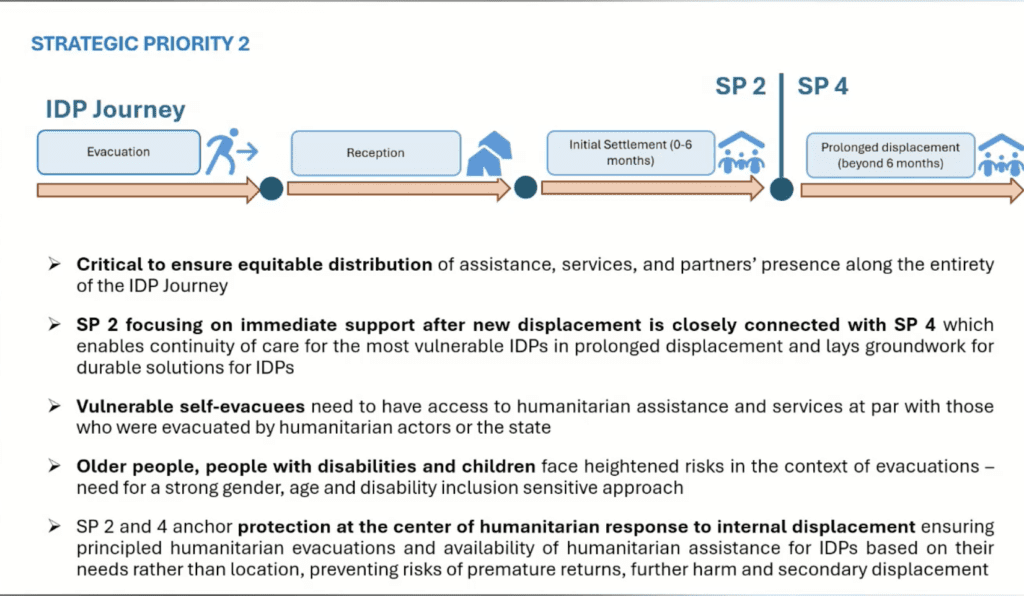
The numbers: In 2025, more than 130,000 people were officially registered as evacuees. The real number? Much higher, because many self-evacuate and don’t register at evacuation centers.
What you need:
Inter-cluster coordination is non-negotiable:
- Cash Working Group
- Social Protection Cluster
- CCCM (Camp Coordination and Camp Management)
- Shelter Cluster
- Health and WASH cluster
Know your local network:
- Temporary dwellings
- Evacuation routes
- Transit centers
Build robust referral pathways:
Your MPCA program shouldn’t exist in isolation. Other agencies and local stakeholders should be able to refer people to you, and you to them. Local coordination isn’t a nice-to-have – it’s a key success factor for 2026.
Element 4: Integrate with Government Social Protection Systems
This is year 5 of the crisis. We’re in protracted crisis territory now. You can no longer afford a blanket, cross-sectional CVA approach. It’s time to integrate with local initiatives and government systems.
Why integration matters:
Ukraine’s government social protection system is robust and launching interesting new programs. If your CVA program isn’t linking with these, you’re missing opportunities for sustainable impact.
Examples of government programs to link with:
Housing Vouchers for IDPs (launched December 2025)
Ministry of Communities and Territorial Development offers vouchers worth nearly 2 million UAH for IDPs evacuated from temporarily occupied territories. This helps them procure apartments or pay mortgages. Right now, it prioritizes IDPs and veterans, but as it scales, more people will access this meaningful long-term support.
Rental Subsidies for IDPs
Another Ministry’s initiative (supported by Ministry of Digital Transformation) provides subsidies for renting apartments, with specific eligibility criteria.
That’s what good CVA looks like:
Element 5: Align CVA with Your Sectoral Strengths
Here’s where it gets interesting: think about how CVA integrates with the help you already provide – in-kind, service provision, capacity building within your sector.
Protection: The Natural Integration Point
For protection actors, integrating cash isn’t a “nice-to-have” – it’s the most natural way of providing support. And I want to be clear: when I say “natural,” I don’t mean simple. I mean logical, aligned with how protection work actually functions.
What this looks like in practice:
Protection-linked cash isn’t the same as blanket MPCA. It’s:
- Tied to case management plans: The cash intervention is part of a broader protection strategy
- Outcome-focused: You’re not just filling a financial gap – you’re enabling someone to move toward safety or stability
- Flexible in amount and timing: A survivor leaving an abusive situation might need a lump sum for relocation. Someone navigating the legal system might need smaller, periodic amounts for fees and transport.
- Complementary to other services: The cash enables people to access the counseling, legal support, or health services you’re already providing or referring them to.
GBV actors are already doing this. If you’re running a GBV program and you don’t have a cash component, you’re probably watching case after case where financial constraints become the barrier to the protection outcome you’re working toward.
Other Sectoral Integration Examples:
If you’re strong in shelter → Winter CVA response might be your program. Help people get through -10°C winters (like right now in Dnipro where I’m writing this). Align with winterization plans for households and institutions.
If you’re in health → There’s plenty of space for sectoral health CVA, especially given:
- Shortages in the pharma supply chain
- Two of the three biggest pharmaceutical providers were targeted in the last 6 months – warehouses completely destroyed
If you in WASH -> consider cash and voucher as an alternative for in-kind support. It is easier said than done, but with carefull design and good nationwide vendors, it is feasible.
Some local actors have successfully implemented vouchers for hygoene products.
Practical health example:
If you’re in the 20km zone (priority number 1 for CVA), prepare for cash-for-health needs. Not all medications are classified as essential or covered by NHSU’s affordable drugs program. Not all are readily available due to pharma supply disruptions.
The Integration Principle:
Whatever your sectoral strength, ask yourself: Where do financial barriers prevent people from accessing the services or outcomes we’re trying to provide?
That’s where CVA fits. Not as a standalone program, but as an enabler of everything else you’re already doing.
The Bottom Line
These five elements aren’t theoretical. They’re based on five years of designing and implementing CVA in one of the most complex humanitarian contexts in the world.
2026 is the year to get smarter – more targeted, more integrated, more coordinated. The funding landscape has fundamentally shifted. The numbers tell the story: from 88% funding in 2022 to 47% in 2025.
Your program design needs to reflect that reality.
The five elements again:
- Design for the 20km frontline zone reality – verify infrastructure, choose cash over vouchers when services are unstable
- Look beyond your comfort zone – prioritize underserved areas like Sumska and Chernihivska oblasts
- Prepare for evacuations and coordinate – build referral pathways and inter-cluster coordination mechanisms
- Integrate with government systems – link with housing vouchers, rental subsidies, NHSU programs
- Align CVA with your sectoral strengths – especially protection (case management), shelter (winterization), and health (pharma disruptions)
These aren’t just recommendations – they’re survival strategies for doing effective CVA work in a constrained funding environment.
Leave a Reply