Key findings
Cash transfers to offset transportation costs substantially increased referral completion among rural conflict-affected beneficiaries. The intervention effectively eliminates one of the most significant barriers to accessing higher-level medical care.
The influence of service cost was secondary and did not meaningfully alter completion rates. The program demonstrates a strong, measurable impact and supports the continued integration of CVA into IMT referral pathways.
Abbreviations & Definitions
- IMT — Integrated Mobile Team
- CVA — Cash and Voucher Assistance
- EER — External Electronic Referral (NHSU e-referral system)
- EER+ — Referral issued via the NHSU e-referral system (service cost fully covered by NHSU)
- EER− — Referral not issued via the NHSU e-referral system (patient pays out-of-pocket for service)
- Positive referral — The beneficiary received the referred service and the referral status is marked Positive in the tracker.
- Negative referral — The beneficiary did not receive the referred service and the referral status is marked Negative in the tracker.
- Completed referral (analysis set) — A referral with a final status (Positive/Negative) after the scheduled follow-up window, per rules below.
Background
In rural conflict-affected areas of Ukraine, transportation barriers significantly impede access to referred medical services. Integrated Mobile Teams (IMTs) reported that patients often cannot reach higher-level care due to lack of public transport and high travel costs. To address this barrier, FHI 360 introduced cash assistance (USD 12–45) to cover two-way transportation costs for eligible beneficiaries.
Objective
To assess whether cash assistance increases the proportion of completed referrals (“Positive referrals”) compared with beneficiaries who received referrals but no cash support. A secondary objective examined whether service cost (free via EER+ vs out-of-pocket in EER−) affects referral completion rates.
Methods
A longitudinal controlled secondary data analysis was performed using IMT referral trackers (30th April–1st November 2025). Completed referrals were categorized as Positive (service received) or Negative (service not received). Outcomes were compared between the cash-assisted group and the non-cash control group and further stratified by EER status. Randomisation at the program level mitigated confounders such as age and disability.
Results:
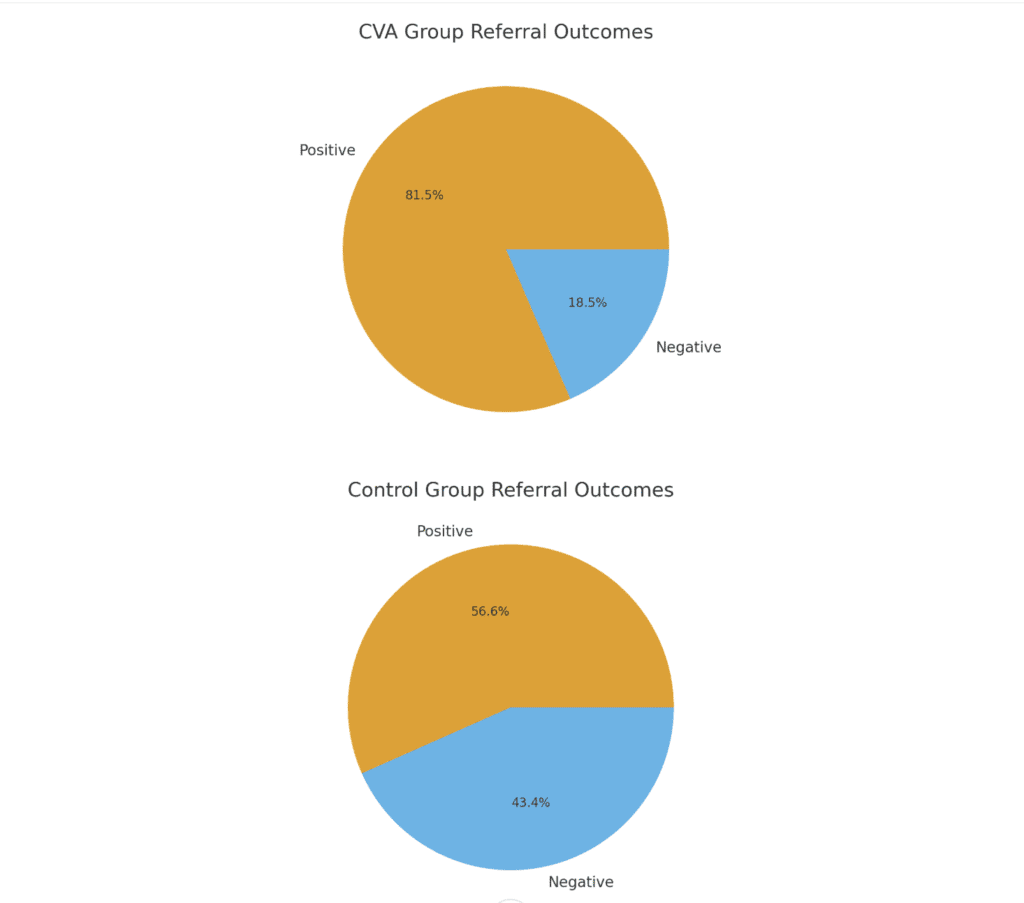
A total of 2,336 completed referrals were analyzed. Cash assistance was strongly associated with improved referral completion:
- CVA group: 81.5% Positive
- Control group: 56.6% Positive
- Risk difference: +24.9 percentage points
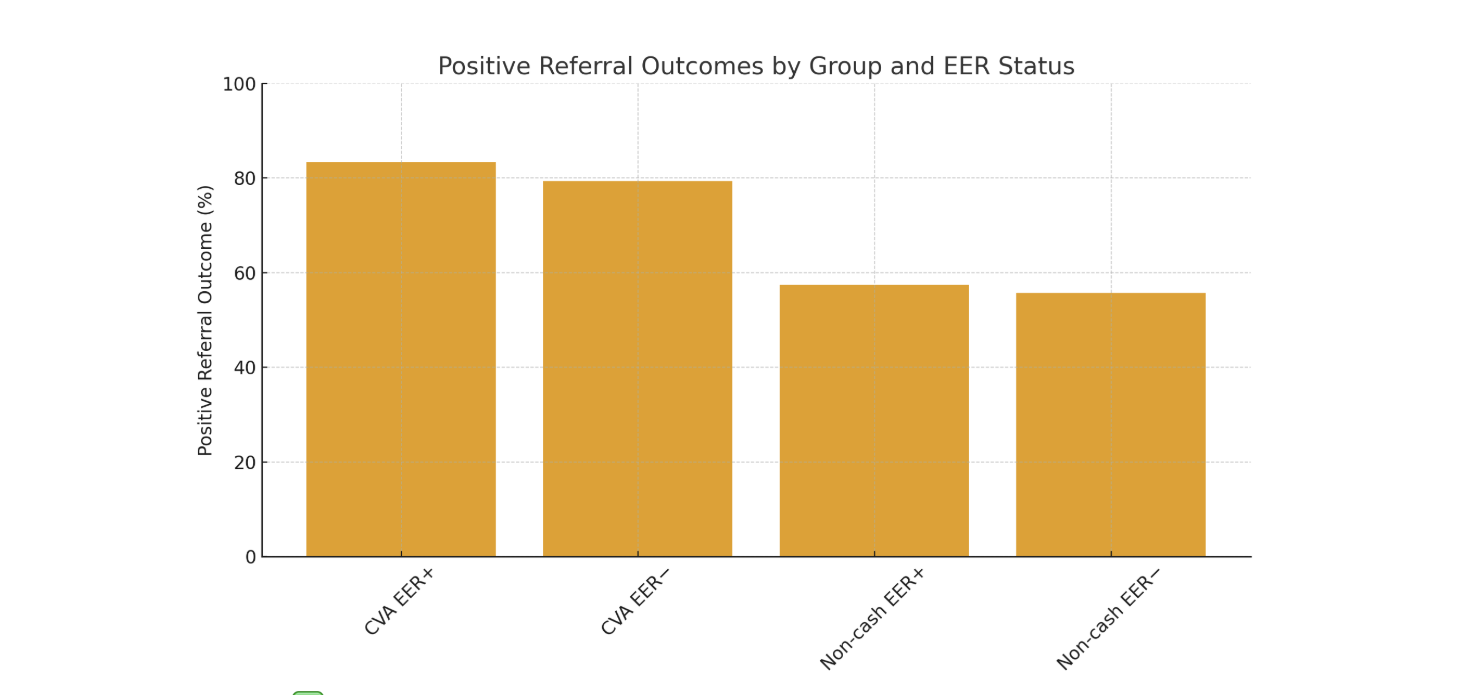
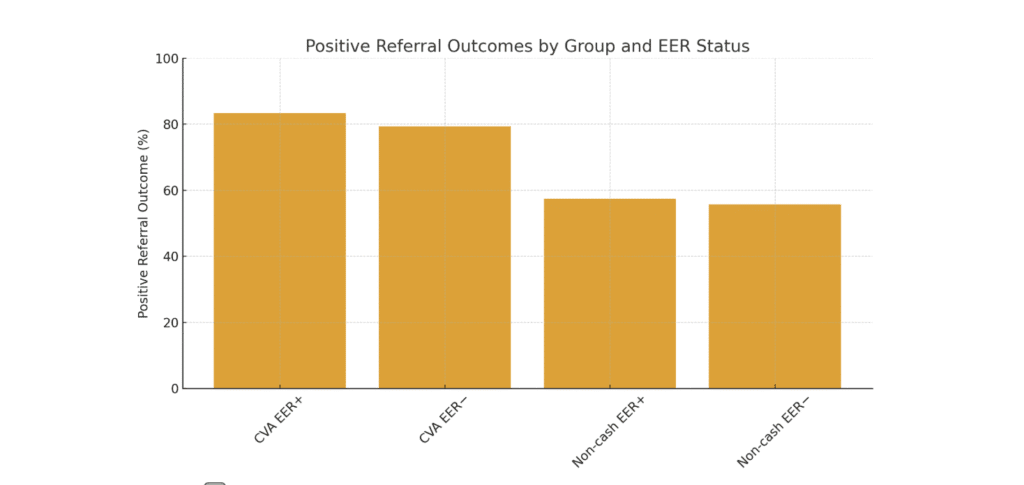
The effect persisted across EER strata:
- Cash + EER+: 83.3% Positive
- Non-Cash + EER+: 57.4%
- Cash + EER−: 79.4%
- Non-Cash + EER−: 55.7%
Service cost (free vs paid) had minimal impact compared to transportation support, confirming that transport—not service fees—is the dominant access barrier.
Study Design and Results
Background & Rationale
Eleven IMTs report transportation cost as a major barrier for rural, conflict-affected beneficiaries to complete referred services (often located in hromada centers or large cities). In frontline areas (Kharkiv, Dnipro, Kherson, Mykolaiv), public transport is scarce/absent. FHI 360 provided CVA (USD 12–45, modality: bank transfer or Ukrposhta) to offset two-way transport. Average CVA lead time: ~1.5 months. Exclusions ensured: (1) no dependency-creating repeated services; (2) referrals clinically justified and evidence-based; (3) pharmacy purchases ineligible; (4) no duplication with other CVA/MPCA.
Objectives
Primary objective:
Compare the proportion of Positive referrals between:
- Investigation group: IMT beneficiaries who received CVA for transport and were referred to higher level of care.
- Control group: IMT beneficiaries who did not receive CVA but were referred to higher level of care.
Secondary objective:
Within each group, compare Positive referral proportions between EER+ vs EER− referrals to assess the additional impact of service cost (free vs paid).
Assumptions
- Transportation is a key barrier; CVA will increase Positive referrals.
- Service costs matter but less than transport; expect smaller or non-significant differences between EER+ and EER− after confirming transport was the primary barrier at eligibility.
Design
Longitudinal, controlled secondary data analysis of IMT referral trackers (SharePoint List + Power Automate).
- Index date (exposure alignment):
- CVA group: date CVA received (not request date).
- Control: referral creation date.
- Follow-up windows:
- Non-CVA: outcome assessed 1 month after referral created.
- CVA: outcome assessed 1 month after CVA received (accounts for ~1.5-month lead time).
- If a service appointment was scheduled but not yet received, perform a short follow-up 3 days after the scheduled appointment date; then finalize status.
- Analysis set: include only Completed referrals (Positive/Negative).
Note: Randomisation is stated to mitigate confounders (e.g., age, disability). We will verify baseline balance and proceed per protocol.
Study Period & Setting
- Planned analysis window: Specify exact 6-month window within April–November 2025 (e.g., April 30th – Nov 1st, 2025).
- Geographic scope: Provide an enclosed list of locations/settlements (IMT catchment areas) across Kharkiv, Dnipro, Kherson, and Mykolaiv oblasts.
- IMTs: 11 teams.
Population, Eligibility & Groups
Inclusion (both groups):
- IMT beneficiary referred to the next level of care within the analysis window.
- Referral tracked in the SharePoint List with required fields completed.
Exclusion (program rules):
- Services requiring repeated/ongoing payments (e.g., chemotherapy, extended physiotherapy).
- Non-evidence-based or non-justified referrals (e.g., massage, acupuncture).
- Pharmacy/medications purchases.
- Duplicate CVA with other cash programs (protection/MPCA).
Group assignment:
- Investigation (CVA): CVA provided for transport (USD 12–45; via bank transfer/UKR POSHTA).
- Control (No CVA): No CVA for transport.
Outcomes
Primary outcome:
- Positive referral proportion = Positive / (Positive + Negative) in each group.
Secondary outcome:
- Stratified Positive referral proportions by EER+ vs EER− within each group; compare differences.
Data Sources & Key Variables
Source: IMT SharePoint referral trackers (Power Automate outputs).
Core fields to extract (minimum set):
- Beneficiary ID (pseudonymized), age, sex, disability flag (if available), location.
- Referral ID, referral date, referred service type, level of care, EER status (EER+/EER−).
- CVA flag (Y/N), CVA request date, CVA received date, CVA amount (USD).
- Appointment scheduled? (Y/N), appointment date.
- Final status (Positive/Negative), finalization date, free-text notes (optional).
- Duplicates/linked cash programs flag (to enforce exclusion).
Data quality checks: completeness of timestamps, logical order (referral → CVA received → follow-up → final status), de-duplication.